- To Change Your Mind - Details Matter
AD/HD: Diagnosis and Treatment Often Miss the Mark
ADD: Predictablity and Irrationality Examined
October 7, 2008ADD Context II: Physics, Reality, and Structure
October 12, 2008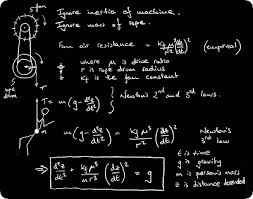
AD/HD, ADD, ADHD – The diagnosis is often missed
Since the diagnosis is missed, treatment objectives are missed even more frequently. – But why?
Example: The Professor Of Physics
Let's take a moment to really look at clinical function – with one example of ADD from an unexpected source: a physics professor.
This will be a short note on a very frequently observed problem:
Our diagnostic grid for ADD Spectrum Disorders [with multiple expressions of attention related issues] is almost purely descriptive – with the inevitable consequence that we most often treat labels, not people. The public is mad because, more frequently than not, our measurements simply don't consider their pain.
ADD involves much more than “hyperactive,” “inattentive” and “combined!” And if you are smart, you must, obviously, be lazy…
In evaluations for ADD/ADHD we don't measure, we don't consider clinically, cognitive function in context – especially if you are really smart! If you are really smart with a bunch of degrees, you couldn't possibly suffer with ADD/ADHD, right?
I have repeatedly witnessed this frequent oversight for years – and that's why I think we should change our perspective, – and why I am busy writing my book. If you see enough brains with SPECT brain imaging, and compare those brains with clinical findings and results from the Conner's Continuous Performance Test [others agree], you will see how that test frequently misses the mark.
What Happens
Many who suffer with ADD show good results on the Conner's CPT – they pass the test, but show classic ADD findings on brain scans and clinically – if you ask the questions more carefully.
Our current criteria for ADD is simply how the patient looks, how they respond to testing in a given context. We know ADD diminishes Pre-Frontal Cortical Function, but we just don't ask the questions that consider brain function.
I have a patient with 2 PhD's and a Master's Degree, about 55 years old [two degrees in physics, and the other in another field of science] – he simply can't think when the variables become unpredictable and, in the context of time, too abundant to manage in a give time frame. He is wonderful in the context of mathematics, but simply can't take the responsibility of working socially with the unpredictable variables present in management with a team.
In math he can think, in “the team” he freezes.
Do you know anyone that has been overlooked like this… just think for a moment.
Why do we miss the details? We are not looking carefully at how to measure, how to consider brain function – and then, one step further, we don't measure the specific reality, the context, of adaptive and maladaptive function. But it's so easy – more coming in the book.
Do leave a comment if you have seen this oversight, – and pass this note along to your friends who have an interest in this frequently overlooked topic!
cp
4 Comments
Betsy-
So true! That *behavioral* wrinkle you describe is so useful, as the behavioral aspect of ADD is so often associated with the bad press, the skepticism, and the negative thinking associated with the diagnosis – it leads the uniformed down the free will direction – “anyone should be able to control their behavior” and move so completely away from the biological elements. “Behavior” is only the surface, “brain function” is what we should be focused upon – therein, thinking first of brain function, and looking at behavior as an expression of the underlying biology, we find ourselves closer to the reality of biology and neurology.
Another quick point on this matter is that so many over on the biology side do miss the psychology, the dynamics of structure in the family as significant.
The best answers are complete and comprehensive, rather than only looking at *one facet* of the spectrum of ADD clinical presentations, as well as the spectrum of ADD causal issues [comorbidity], contributory factors. We really must move away from the one trick pony assessment with brain function – as both biology and psychology contribute to every presentation.
Thanks for your comments-
Chuck
Oh yes. I have seen this and see it often. That AD/HD is fundamentally a cognitive disorder is missed in favor of the easier, more obvious, behavior.
AD/HD is not a behavior disorder. The behavior is many mileposts down the road from the seat of the problem. Its sufferers know that, until they are mischaracterized over years until they go along and forget their earliest perceptions.
So they tend to answer the questions asked instead of saying the questions are the wrong ones. I know a few people who have held onto their own experience and they have often met with skepticism even from their doctors.
Keep up the good work.
Gina,
Thanks for your confirmation of this oft overlooked manifestation – yes, agreed, it seems more the rule than the exception.
Just sent out another post to clarify “context” after someone in another *context* asked me about the meaning of “acuity” – might as well clear things up!
Thanks,
Chuck
I’ve seen this oversight so often it’s more the rule than the exception!
Thanks for bringing this to our (and, I hope, clinicians’) attention, Dr. Parker.
Gina